


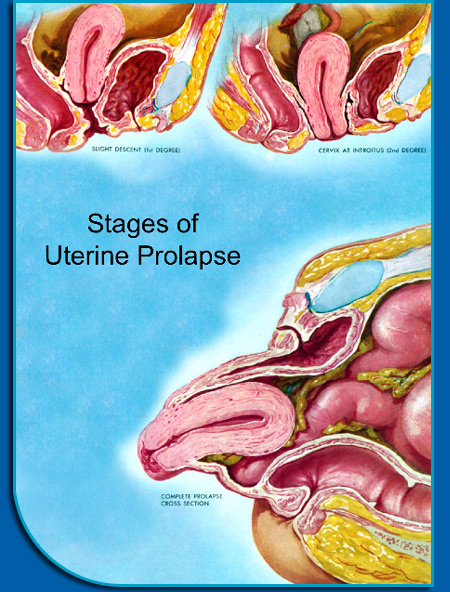
What is Prolapse? |
How is prolapse treated? First, if a patient is not bothered by prolapse, she may not need any treatment at all. In general, treating prolapse is about quality of life. Patients should be reassured that this is common and except in rare situations, can usually be observed without treatment. However, patients should also be reassured that if they are bothered by prolapse or incontinence, there are many treatments available that can help them get back to normal life.There is no reason to live with prolapse or incontinence if it bothers you or affects your quality of life. Nonsurgical treatments Kegel exercises or physical therapy can help strengthen the pelvic muscles. This is helpful with urinary incontinence and may delay the development of prolapse. However, it is unlikely that exercises alone will repair significant vaginal prolapse. Pessaries are removable rubber or silicone devices that can be placed in the vagina to hold the organs in place. Once appropriately fitted, a pessary can be removed and cleaned on a regular basis by the patient for as long as she would like. Pessaries often work well, but the prolapse will likely return if pessary use is stopped. Therefore, we recommend pessaries for young woman who may want to have more children, women who have a medical condition that makes surgery inadvisable, or for women who would like to post-pone surgery for some period of time – perhaps to take care of an ill family member or when it may be more convenient for her schedule. There are also several ways to surgically treat prolapse – many of which are minimally invasive. In general, the options that will be offered to a woman will depend on the training and experience of the surgeon. There is no one right answer for all patients. We suggest a consultation with a fellowship-trained urogynecologist to determine which option is best for each patient. Click HERE for a description of the different types of surgeries for prolapse repairs. |
 |